What makes a good life? Health? Wealth? Or maybe good interpersonal relationships?
Whilst we could argue that people value different things, most of us also want similar things. To be able to choose and make decisions about the way we live, to be loved and valued by people around us and to have the skills and means to achieve our goals.
The quality of life of people with intellectual and developmental disabilities, however, has been non-existent for many years. Historically, this population was subject to years of institutionalisation and practices that we now consider abuse. The period of institutionalisation, which in the UK only started shifting in the ‘80s led to attempts to conceptualise quality of life specifically for this population.
According to Dr Bob Shalock, the Quality of Life for a person with an intellectual or developmental disability has the same characteristics as for every human being. However, this population is statistically at risk of experiencing reduced quality of life.
A central part of support teams within the context of government policies such as The Care Act (2014) is to enhance people’s quality of life by enabling choice, control and social inclusion.
Shalock described eight domains for Quality of Life. These domains are:
- Emotional well-being: contentment, self-concept, lack of stress.
- Interpersonal relations: interactions, relationships, supports.
- Material well-being: financial status, employment, housing.
- Personal development: education, personal competence, performance.
- Physical well-being: health and health care, activities of daily living, leisure.
- Self-determination: autonomy, personal control, personal goals, choices.
- Social inclusion: community integration and participation, roles, supports.
- Rights: legal, human, respect, dignity, equality.
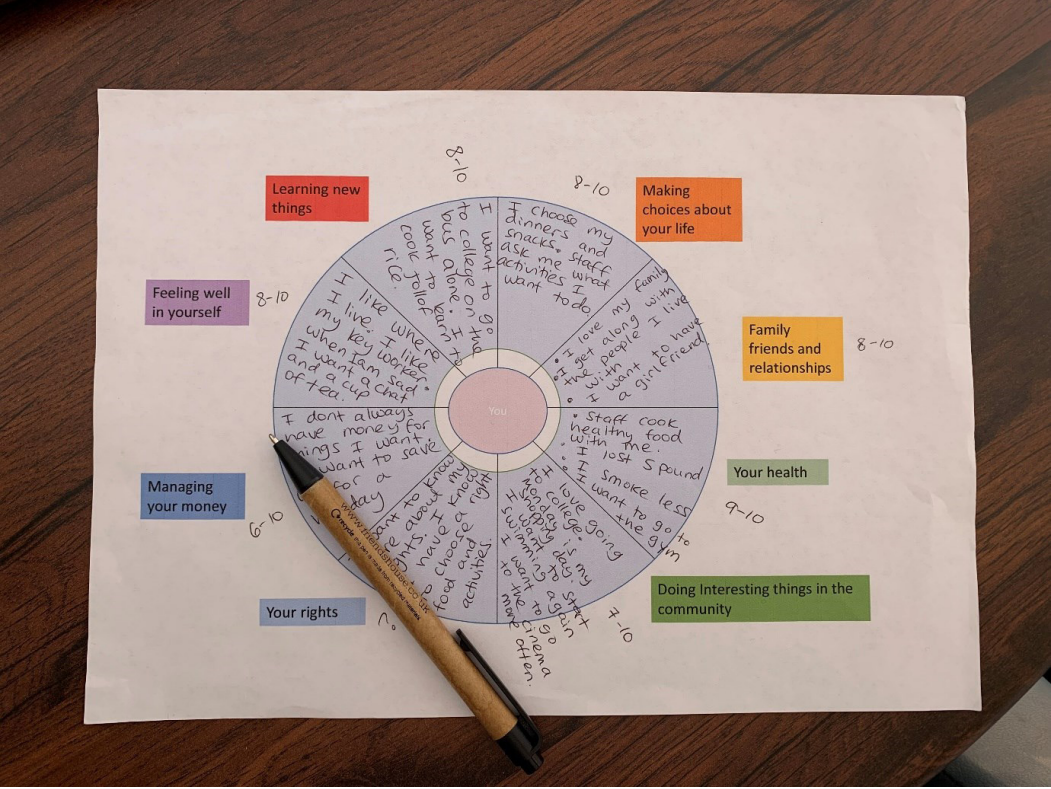
At Liaise a significant role of the in-house multidisciplinary team is to lead on Quality-of-life enhancement. We use our professional knowledge and communication expertise to involve people in the Quality-of-life reviews and assessments. Some Quality-of-Life assessments use objective measures for example looking at living conditions, while other processes are adapted to encourage the person to air their views and determine their own life goals and wishes. Based on Shalock’s quality of life domains we developed a visual tool, which allows people to reflect on different aspects of their life and assist the support staff to deliver person-centred care. In this process, the person may be asked to rate an area of their life from 0-10 and reflect on what is going well and what is missing. Those with less cognitive or communication skills are supported by pictures and simpler language.
This process ensures that we listen to and act upon what is important to the person and avoid focusing solely on what the team considers important for them. One of the people we support commented about the process and said: “it was good to be asked these questions in this way. It helped me figure out what I want to do and not just things the staff want me to do, like my personal care.”
It is worth noting the evidence-based link between good quality of life and reduction in behaviours of concern. Quality of life enhancement, therefore, affects the whole service and support us to deliver excellent care.